
On 27th November, Indian Twitter developed cardio-phillia. The Indian Express published a story about judge BH Loya’s death which sort of contradicted findings in the Caravan Magazine.
Now the moment the Indian Express counter came, expectedly the Left Wing twitter was abuzz with conspiracy theories.
So after Modi’s fake degree, emerges the fake ECG report of Judge Loya.
Heart attack date 1 Dec.
ECG date 30 Nov. pic.twitter.com/WdKY78mnck— Kapil (@kapsology) November 27, 2017
IE puts out an ‘investigative’ story to put lid on murky death of Judge Loya dealing with Amit Shah murder trial.Puts out an ECG done at govt hosp which is dated 30/11 when the judge was supposed to have been taken there in 1/12!Does not talk to judges who were with Loya.Cover up https://t.co/d4KvpAKHVO
— Prashant Bhushan (@pbhushan1) November 27, 2017
So I just got on to this Twitter thread by a journalist, where the favourite topic of discussion/outrage of the day was ECG of Loya .
Beta .. I get my ECG done every 3 months ..
All reports show ECG in Local Time only ..
Last year, was hospitalized overseas ..
They also did ECG .. Date and TIme shown was Local ..
Don’t bring in “US” in everything
ECG machine is not Language setting of Windows#BhagYahaSe https://t.co/oUaZlBy4Vb— Shuvankar Mukherjee (@shuvankr) November 27, 2017
The claims by this journalist were :
- ECG was normal
- Time/date was wrong and it was not possible
- It was a fake/manufactured ECG .
I protested, of course.
And your confidence in ECG changes at time of CPR on basis of getting ECGs every three months is to be applauded..It is simply amazing that they could fake a suggestive ECG(much more difficult) n forget to fake the date (relatively easy, manually enter in machine).
— anupam (@anupampom) November 27, 2017
What happened next was totally amusing and peak twitter-
- I got abused for being a fake/troll doctor
- some body who gets ECG quarterly, boasted of being admitted in US has/is an advertiser all advised me some with # chal bhaag hashtag
Now thankfully I am an MD (medicine), have been working in cardiology for three years at a CCU. I am USMLE certified (US license) and have practised and worked in New york city for 1 year as a medicine resident.
Basically the only thing I didn’t have which these twelebs did, was confidence and power of snark. Shows the hollowness of many of these twelebs.
Indian express in due time offered following clarification :
Update by @IndianExpress on the ECG anomaly question raised by @thecaravanindia journalists. Dr @anupampom, MD Cardiology, was correct in his assessment. pic.twitter.com/Bcgezlw4Gf
— Anand Ranganathan (@ARanganathan72) November 27, 2017
Dr Ranganathan himself put up some great counters that included Medical and non medical facts.
4/4 It becomes clear from @IndianExpress fact-check that, if as insinuated by @thecaravanindia, Justice Loya was murdered, then not only the entire medical, official, police, and administrative machinery, but also, and most crucially, *half a dozen judges*, are complicit. Well. pic.twitter.com/CjxzkUaPR5
— Anand Ranganathan (@ARanganathan72) November 27, 2017
I am also weighing in on the subject as a Medical professional by answering some questions that may be asked about this entire ECG controversy.
- Is ECG normal ?
ECG was abnormal. (ST depression in 1, aVL , hyperacute T waves in v2,V3,V4) . V1 seems to disconnected. Appears to be Acute coronary syndrome (STEMI mimic- Hyperacute T waves) within window period. In the setting of persistent retrosternal chest pain, patient should be given aspirin, sorbitrate, atorvastation, clopidogrel, ideally should be referred to a higher centre with PCI/thrombolysis facility.
- Why is date/time wrong 30/11 6.11 when it is claimed that ECG was done at 4.45-5 AM on 1st december.
Date/time was obviously wrong, but it is possible because ECG machines imported from USA often get reset and technician doesn’t bother to enter ECG manually because of a combination of laziness/emergency. Also the time 6.11 in US EST was suspiciously closer to 4.41 IST. People objected AM/PM was not mentioned but often there is an option of entering 12 hour format which is the default in many machines i work in my set up.
- How are you so sure Sanghi ?
I am only offering a potential cause. Case records, Doctor testimony are gold standards in these cases instead of single ECG with misprints as I mentioned
- This is ECG of another patient – Faker/Feku ?
Yes title is wrong, written with pen. But time/date are easiest things to “fix” than an ECG with 12 leads with ECG showing abnormality. If I were to fix I would manually type name proper date and time to correct order of seconds and pick up full blown MI (few doctors on twitter got it wrong too) from an already admitted patient.
An old medical joke goes like
Question : Give me an example of double-blind randomized clinical trial?
Answer : Pick two Orthopedicians at random and get them to read an ECG.
The moot point is correct recognition of Acute coronary syndromes is uncommon and hence even medical doctors struggle with it, leave alone laymen.
- OK. How often are these date/time/name anomalies in common practice ?
I see them in 60-70% ECGs in my set up a busy government hospital. I interpret 25-40 ECGs every day. Most of them are referrals from outside. In chest pain emergencies the figure with either wrong date/time/name is even higher. In yesterday night call, none of the ECGs had all of three date/time/name correctly entered. I have worked in different Indian hospitals and unfortunately you have to take my word for it. If one can confirm with other doctors, they would probably say the same. The first thing we are trained in ER is to verify time of all such documentation with patient concerned more so in acute coronary syndrome as there is a window period for PCI/thrombolysis intervention.
- But would not this be treated as flimsy evidence in courts ?
Ideally date/time should be entered correctly in any medico-legal case. It is often not done and entered manually. That is why case sheet and doctor testimony is the GOLD STANDARD even in courts. You can also ask Dande Hospital for some previous ECGs of the day -but in my opinion it all boils down to trust on doctor/hospital set up.
- But case sheet is written by pen as well, can it be fudged easily ?
Well, ideally we need digitally written notes with EMR, which would be difficult to alter and leaves timestamps. 99% of hospitals in India don’t have electronically written daily notes. Not even high-end corporate hospitals in India. So eventually you have to trust the doctors.
- I am still suspicious. Is there any way to resolve this quagmire ?
Yes. Meditrina Hospital which administered DC shock during CPR – must be having other set of ECGs. Pre DC shock and flat line for death. Since the ECGs are old you might get a print out. Death certificate should be there with correct details.
However if you already believe everything is fudged. Why bother?
- Was Dande Hospital right in referring patient without a doctor ?
Ideally such cases should be accompanied with a doctor and medical ambulance often not available in Indian scenario. However in STEMI mimics time is muscle door to needle or thrombolysis time should be less than 90 minutes.
- Why was autopsy done?
Many a times tertiary hospitals insist on autopsy if it is a high-profile case. Nobody wants to pick up dead body
- You are saying repeatedly that case records clinical history and examination (notes) are a critical evidence in this case. If so why do ECG at all. Why are you bluffing ?
Short answer :
No investigation/test can be divorced from its clinical context. It is a critical part of medicine, one of the reasons computers have not replaced humans in management of chest pain and it won’t be happening anytime soon. Even though they started “reading” ECG better than humans almost 30 years back. In other words in medicine, context is the king.
Long answer :
In Chest pain emergencies – a single normal ECG misses the diagnosis up to 50% of the times. That is why the recommendation is to get three sets of ECG and three sets of cardiac enzymes at 0,6,12 hours since start of severe chest pain (defined as peristing greater than 30 minutes,+- mid-sternal+- radiation) to be sure that heart attack is effectively ruled out.
Suppose the ECG (which I would call moderately abnormal is judge Loya’s case) was normal. Could the doctor have ruled out heart attack if it was normal as some twitterattis and even some docs to my surprise, were claiming? The answer is no. He would still have to run the protocol to be sure. However the Doctor on duty in Dande hospital is to be commended for picking up this ECG early (in retrospect he was right because Dr. Loya collapsed 1 and a half hours later)
One of the reasons most US hospitals have telemetry units that will hold you up to 12 hours to be effectively sure. Even if you visit resource-constrained Indian hospitals they will do 2-3 sets of ECG and cardiac enzymes to effective rule out heart attack.
Have you ever wondered why chest pain is the most common symptom given by politicians when they are about to go to jail – one is obvious stress, second important factor is that it will assure a hospital stay of at least 12 hours.
Not only in unstable patients, context is very important in stable patients as well. Lets discuss a famous example given by Nassem Taleb in his book ‘Fooled by Randomness’.
Even if a test has only 5% false positive rate, and 0% false negative rate, the odds that you have a certain disease will only be 2% even if the test is positive in populations/patients with low base-rate (1/1000). The base rates in medicine are determined from a doctor’s experience, patient’s history and patient’s examination – A critical part of what we do. This is called Bayes Theorem. See more examples about use of Bayes theorem in Jesus miracles and the Famous Taxi-cab problem by nobel-prize winners Tversky and Kahneman.
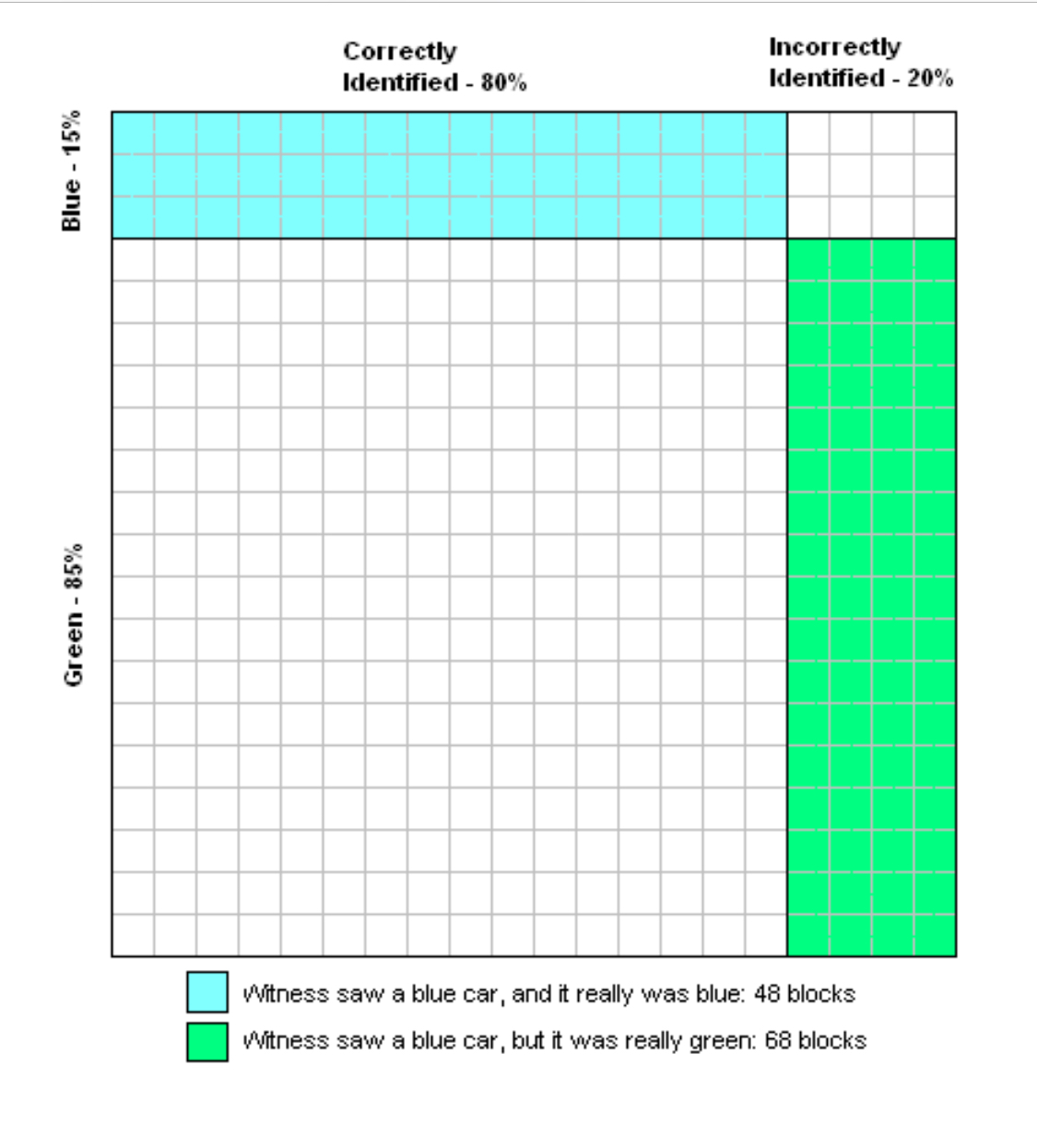
A cab was involved in a hit and run accident at night. Two cab companies, the Green and the Blue, operate in the city. 85% of the cabs in the city are Green and 15% are Blue.
A witness identified the cab as Blue. The court tested the reliability of the witness under the same circumstances that existed on the night of the accident and concluded that the witness correctly identified each one of the two colors 80% of the time and failed 20% of the time.
What is the probability that the cab involved in the accident was Blue rather than Green knowing that this witness identified it as Blue?
Most subjects gave probabilities over 50%, and some gave answers over 80%. The correct answer, found using Bayes’ theorem, is lower than these estimates:
There is a 12% chance (15% times 80%) of the witness correctly identifying a blue cab.
There is a 17% chance (85% times 20%) of the witness incorrectly identifying a green cab as blue.
There is therefore a 29% chance (12% plus 17%) the witness will identify the cab as blue.
This results in a 41% chance (12% divided by 29%) that the cab identified as blue is actually blue.
Medical evidence synthesis with prior knowledge and data from tests is a very important part of what we do as Cardiologists. The symptoms type of angina (chest pain) is used to determine what is the base-rate in that population and the result of the test is used to update that probability.
In my practice, I regular use this tests in a self-coded pre-test calculator diagnosing coronary artery disease and have coded in a medical software that I wrote in my TMT lab, as do most of the doctors though more intuitively and perhaps in a less mathematical fashion. This wonderful New York times article talks about other uses of Bayes theorem from interpretation of clinical trials to law
In summary, you can’t interpret that ECG in isolation, case history, medical records are the most important part of medicine and will be the first piece of evidence that should be discussed as part of diagnosis in courts or in medical ward rounds for that matter.
12 . Which paper should we trust, Caravan or Indian Express ?
Both papers erred , While Indian express story erred in not querying the hospital at the time about date/time mis-match on ECG on first print(they issued a clarification later) leading to all conspiracy theories, the Caravan journalists did an extremely shoddy job of not talking to doctors/hospital at all. They claimed there wasn’t even an ECG, without due diligence. If you are out-sourcing even fact-gathering or a basic fact-check to readers then what is the purpose of your existence apart from being an instrument of politics or a medium to carry advertisement as your critics often accuse you of.
As a doctor, I wish more editors would hold these journalist to the same standards as they expect from us doctors. If we would misreported the aforesaid ECG or fail to ask for a clinical clue at all, in medicine it often means a life lost. In media-space that is perhaps loss of credibility for journalism fraternity as a whole.
(This article was originally published on on author’s blog)
